
- 首页 > 正文
ASCO GI国际视角|肝癌治疗进展速递:两项研究同证免疫联合方案治疗获益
发表时间:2026-03-07 10:51:10
编者按
肝细胞癌(HCC)是临床常见的原发性肝脏恶性肿瘤,多数患者确诊时已进展至中晚期。经动脉化疗栓塞(TACE)是目前中期HCC的标准治疗方案,但其疗效仍有局限。在2026年美国临床肿瘤学会胃肠道肿瘤研讨会(ASCO GI)上,德国美因茨大学医学中心的Peter Robert Galle教授报告了两项重要研究:IKF-035/ABC-HCC研究(摘要号478),评估了阿替利珠单抗联合贝伐珠单抗对比TACE治疗中期HCC患者的疗效;CheckMate 9DW研究(摘要号LBA479),公布了纳武利尤单抗联合伊匹木单抗在不可切除HCC一线治疗中长达4年的随访结果。这两项研究为HCC的系统治疗提供了重要证据。《肿瘤瞭望消化时讯》将深入解读其研究背景与关键结果,以期为临床实践提供参考。
《肿瘤瞭望消化时讯》在2026 ASCO GI现场报道
研究一
中文标题:IKF-035/ABC-HCC——阿替利珠单抗联合贝伐珠单抗对比TACE治疗中期HCC的Ⅲb期、随机、多中心、开放标签试验
英文标题:IKF-035/ABC-HCC: A phase Ⅲb, randomized, multicenter, open-label trial of atezolizumab plus bevacizumab versus transarterial chemoembolization (TACE) in intermediate-stage hepatocellular carcinoma
摘要号:478
研究背景
HCC是全球范围内最常见且致死率最高的恶性肿瘤之一。TACE作为局部治疗手段,是目前中晚期(BCLC B期)HCC的标准治疗方案。IMbrave150 Ⅲ期研究表明,对于TACE治疗失败或不适合TACE的晚期和中晚期HCC患者,抗PD-L1抗体阿替利珠单抗联合抗VEGF抗体贝伐珠单抗的一线治疗方案较索拉非尼可延长生存期,并因此被批准用于该适应症。然而,对于原本应按标准方案接受TACE治疗的中期HCC患者,阿替利珠单抗联合贝伐珠单抗是否优于TACE尚不明确。尽管已有若干试验正在评估TACE联合系统治疗对比单纯TACE的获益差异,但ABC-HCC试验直接比较了阿替利珠单抗联合贝伐珠单抗及系统治疗对比TACE的疗效和安全性。本研究采用分组序贯设计,计划在信息成熟度达到33%和66%时进行两次中期分析,以评估疗效/无效性。
研究方法
ABC-HCC是一项国际、多中心、随机、开放标签、由研究者发起的Ⅲb期临床试验,旨在直接比较阿替利珠单抗联合贝伐珠单抗对比TACE在中期HCC或经主治医师判断具有TACE适应证的HCC患者中的疗效。研究计划纳入320例确诊HCC患者,入选标准包括:不适合根治性手术/消融或肝移植,但适合TACE治疗;无肝外转移;无大血管侵犯(Vp1/2型门静脉侵犯除外);ECOG评分≤1;Child-Pugh分级为A级或B7级。患者按1:1随机分配接受系统治疗(A组:阿替利珠单抗,1200 mg静脉注射;贝伐珠单抗,15 mg/kg静脉注射;每3周一次;最长治疗24个月)或TACE治疗(B组:按需进行,由研究者评估认为可继续接受TACE时再进行)。每8周进行一次影像学检查(CT/MRI),以评估主要终点“治疗策略失败时间”(TTFS:从随机分组到死亡或需要其他治疗方案的时间)。本研究报告了在33%信息成熟度时进行的首次疗效/无效性中期分析结果。
研究结果
截至数据分析时,已在奥地利、法国、德国、印度、意大利、日本和西班牙的54个研究中心入组206例患者。在数据截止日期,共有194例患者完成随机分组,其中168例患者随访时间≥3个月,被纳入本次中期分析(A组:87例;B组:81例)。在主要终点TTFS方面,共记录到100起事件(A组:44例;B组:56例)。系统治疗组的中位TTFS为14.6个月,TACE治疗组为9.5个月(HR=0.55;95%CI:0.36~0.83)。基于上述结果,本研究将继续进行。
研究结论
首次中期分析的结果为评估阿替利珠单抗联合贝伐珠单抗对比TACE在中期HCC患者中的疗效提供了重要依据,并提示在TTFS方面,系统治疗可能优于TACE。基于该发现,本研究将推进至66%信息成熟度(169例事件)时的第二次中期分析[1]。
研究者说
关于IKF-035/ABC-HCC研究,亚组设计在入组时已考虑肿瘤负荷、病灶数量和肝功能分层等因素,这些信息将通过次要终点或描述性分析收集。对比TACE,阿替利珠单抗联合贝伐珠单抗在中期HCC患者中的主要临床获益,目前首次中期分析结果尚不完全,我们预期将在包括OS在内的终点中观察到优效性。基于现有结果,该研究可能促使临床实践中更多BCLC B期患者接受联合治疗。
研究二
中文标题:纳武利尤单抗联合伊匹木单抗对比仑伐替尼或索拉非尼一线治疗不可切除HCC:CheckMate 9DW试验的4年随访结果
英文标题:Nivolumab plus ipilimumab vs lenvatinib or sorafenib as first-line treatment for unresectable hepatocellular carcinoma (HCC): 4-year follow-up of CheckMate 9DW
摘要号:LBA479
研究背景
在CheckMate 9DW研究(NCT04039607)预先设定的中期分析中,中位随访35.2个月的结果显示,在未经治疗的不可切除HCC患者中,纳武利尤单抗联合伊匹木单抗(NIVO +IPI)较仑伐替尼或索拉非尼(LEN/SOR)显著延长了总生存期(OS)(HR=0.79;95%CI:0.65~0.96;P=0.0180),客观缓解率(ORR)更高(36% vs. 13%,P<0.0001),且缓解持续时间更长,安全性良好[2]。基于这些结果,NIVO+IPI联合方案已获得美国FDA、欧盟委员会及其他国家批准,作为不可切除HCC的一线治疗方案。本文报告了中位随访4年的最新疗效和安全性结果。
研究方法
本研究纳入经组织学确诊、既往未接受过系统治疗的晚期HCC成年患者,这些患者不适合接受或经根治性手术/局部区域治疗后疾病进展,根据RECIST v1.1标准,未治疗病灶≤1个,Child-Pugh评分为5或6分,ECOG体能状态评分为0或1分。患者按1:1的比例随机分组,分别接受NIVO 1 mg/kg+IPI 3 mg/kg每3周一次(最多4个周期)治疗,随后接受NIVO 480 mg每4周一次治疗,或由研究者选择SOR 400 mg每日两次或LEN 8 mg或12 mg每日一次治疗,直至疾病进展或出现不可耐受的毒性反应。NIVO的给药时间最长为2年。主要终点为OS;次要终点包括由盲态独立中心评估(BICR)的ORR和缓解持续时间(DOR)。
研究结果
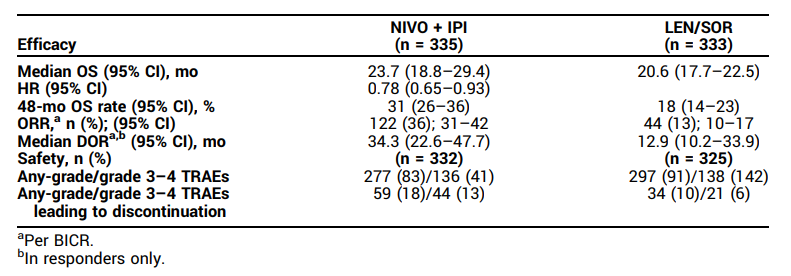
共有668例患者随机分配至NIVO+IPI组(n=335)或LEN/SOR组(n=333);在LEN/SOR组的325例患者中,275例(85%)接受了LEN治疗。经过52.5(44.0~66.1)个月的中位随访后,NIVO+IPI方案与LEN/SOR方案相比,持续显示出OS获益(HR=0.78;95%CI:0.65~0.93),且48个月OS率更高(31% vs. 18%)。NIVO+IPI方案的ORR高于LEN/SOR方案(36% vs. 13%),完全缓解率也更高(分别为8% vs. 2%),且DOR更长(中位DOR分别为34.3个月 vs. 12.9个月)(表1)。治疗相关不良事件(TRAE)的汇总见表1。
表1. 研究结果
研究结论
经过4年的随访,一线NIVO+IPI方案在不可切除的HCC治疗中持续表现出优于LEN/SOR方案的疗效获益,且安全性可控,未出现新的安全性问题。上述结果进一步支持NIVO+IPI方案作为此类患者的标准治疗方案[3]。
研究者说
开展CheckMate 9DW研究并设置4年随访期,主要是考虑到目前仍有相当一部分患者对Imbrave150或Himalaya方案无应答,存在未被满足的临床需求。在长期随访中,纳武利尤单抗联合伊匹木单抗的关键生存数据显示,4年总生存率达31%,相较于对照组的18%表现突出。在安全性方面,未观察到新的不良事件,免疫相关不良事件通常较早发生,长期管理未见新增风险。这些长期结果进一步确认了该联合方案在不可切除HCC一线治疗中的良好疗效和可靠安全性,为临床实践提供了重要依据。
参考文献:
[1] Peter Robert Galle, et al. 2026 ASCO GI. Abstract 478.
[2] Yau T, et al. Lancet. 2025 May 24;405(10492):1851-1864.
[3] Peter Robert Galle, et al. 2026 ASCO GI. Abstract LBA479.
Abstract 478摘要原文
IKF-035/ABC-HCC: A phase Ⅲb, randomized, multicenter, open-label trial of atezolizumab plus bevacizumab versus transarterial chemoembolization (TACE) in intermediate-stage hepatocellular carcinoma
BACKGROUND:
Hepatocellular carcinoma (HCC) is among the most common and deadliest cancers worldwide. Locoregional treatment (LRT) with transarterial chemoembolization (TACE) is standard of care (soc) for intermediate stage (BCLC B) HCC. The IMbrave150 phase 3 study demonstrated that combination of the anti-PD-L1 antibody atezolizumab and the anti-VEGF antibody bevacizumab (atezo/bev) extends survival compared to sorafenib in first-line treatment of advanced and intermediate stage HCC failing/unsuited for TACE which has led to its approval in this setting. However, it is unknown if atezo/bev is more efficacious than TACE in patients with intermediate stage HCC patients who would be treated with TACE per soc. While several trials assess the benefit of adding systemic therapy to TACE vs. TACE alone, the ABC-HCC trial directly compares the efficacy and safety of systemic treatment with atezo/bev vs. TACE. ABC-HCC is using a group sequential design with two planned interim analyses (IA) at 33% and 66% information time to assess efficacy/futility.
METHODS:
ABC-HCC is an international phase 3b, randomized, multicenter, open-label, investigator-initiated trial directly comparing atezo/bev vs. TACE in intermediate stage HCC or HCC with indication for TACE according to the treating physician. 320 patients with confirmed HCC (not amenable to curative surgery/ablation, liver transplantation, but amenable to TACE, no extrahepatic spread, no macrovascular invasion except for Vp1/2, ECOG ≤ 1, Child-Pugh A/B7) are randomized (1:1) to receive either systemic treatment (Arm A: atezo, 1,200 mg IV; bev, 15 mg/kg IV; Q3W; max. 24 months) or TACE (Arm B: on demand as long as TACEable as assessed by the investigator). Imaging (CT/MRI) is performed Q8W to determine the primary endpoint time to failure of treatment strategy (TTFS: Time from randomization until death or need for a further therapeutic option). Here, we report on the first efficacy/futility IA at 33% information time (85 events).
RESULTS:
To date, 206 pts have been enrolled at 54 centers in Austria, France, Germany, India, Italy, Japan and Spain. At data cut-off (06/13/2025), 194 pts were randomized, of whom 168 pts had a follow up duration of ≥ 3 months and were included in the IA (Arm A: 87; Arm B: 81). 100 events were observed for the primary endpoint TTFS (Arm A: 44; Arm B: 56). Median TTFS was 14.6 months in Arm A vs. 9.5 months in Arm B with a HR of 0.55 (95% CI [0.36, 0.83]). Based on these results, the trial was continued.
CONCLUSIONS:
The results of the first IA provide important insights into the efficacy of atezo/bev vs. TACE in intermediate stage HCC and suggest a superiority of systemic therapy compared to TACE in regard to TTFS. Based on these findings, the trial is progressing to the second IA at 66% information time (169 events).
BACKGROUND:
At a preplanned interim analysis of CheckMate 9DW (NCT04039607), with 35.2 months of median follow-up, nivolumab plus ipilimumab (NIVO + IPI) demonstrated significant overall survival (OS) benefit vs lenvatinib or sorafenib (LEN/SOR) (hazard ratio [HR] 0.79 [95% CI, 0.65-0.96]; P = 0.0180), higher objective response rate (ORR; 36% vs 13%, P < 0.0001) with durable responses, and manageable safety in patients (pts) with previously untreated unresectable HCC (Yau T et al. Lancet 2025;405:1851-64). Based on these results, NIVO + IPI combination was approved as a first-line (1L) treatment for unresectable HCC by the US FDA, European Commission, and in other countries. We report updated efficacy and safety results at a median follow-up of 4 years.
METHODS:
Adults with previously untreated histologically confirmed advanced HCC, either ineligible for or having progressed after curative surgical/locoregional therapies, ≤ 1 measurable untreated lesion per RECIST v1.1, Child-Pugh score 5 or 6, and ECOG performance status 0 or 1 were included. Pts were randomized 1:1 to receive NIVO 1 mg/kg + IPI 3 mg/kg Q3W (up to 4 cycles) followed by NIVO 480 mg Q4W or investigator's choice of SOR 400 mg BID or LEN 8 mg or 12 mg QD until disease progression or unacceptable toxicity. NIVO was given for a maximum of 2 years. The primary endpoint was OS; secondary endpoints included ORR and duration of response (DOR) per blinded independent central review (BICR).
RESULTS:
A total of 668 pts were randomized to NIVO + IPI (n = 335) or LEN/SOR (n = 333); among 325 pts treated in the LEN/SOR arm, 275 (85%) received LEN. After a median (range) follow-up of 52.5 (44.0-66.1) months, NIVO + IPI continued to show OS benefit vs LEN/SOR (HR, 0.78; 95% CI, 0.65-0.93), with higher 48-month OS rates (31% vs 18%; Table). ORR was higher with NIVO + IPI vs LEN/SOR (36% vs 13%), with higher complete response rates (8% vs 2%, respectively) and durable responses (median DOR, 34.3 vs 12.9 months, respectively; Table). A summary of treatment-related adverse events (TRAEs) is shown in the Table.
CONCLUSIONS:
After 4 years of follow-up, 1L NIVO + IPI continued to show sustained efficacy benefit vs LEN/SOR in unresectable HCC and manageable safety with no new concerns. These results continue to support NIVO + IPI as a standard-of-care treatment in these patients.
肝细胞癌(HCC)是临床常见的原发性肝脏恶性肿瘤,多数患者确诊时已进展至中晚期。经动脉化疗栓塞(TACE)是目前中期HCC的标准治疗方案,但其疗效仍有局限。在2026年美国临床肿瘤学会胃肠道肿瘤研讨会(ASCO GI)上,德国美因茨大学医学中心的Peter Robert Galle教授报告了两项重要研究:IKF-035/ABC-HCC研究(摘要号478),评估了阿替利珠单抗联合贝伐珠单抗对比TACE治疗中期HCC患者的疗效;CheckMate 9DW研究(摘要号LBA479),公布了纳武利尤单抗联合伊匹木单抗在不可切除HCC一线治疗中长达4年的随访结果。这两项研究为HCC的系统治疗提供了重要证据。《肿瘤瞭望消化时讯》将深入解读其研究背景与关键结果,以期为临床实践提供参考。
《肿瘤瞭望消化时讯》在2026 ASCO GI现场报道
研究一
中文标题:IKF-035/ABC-HCC——阿替利珠单抗联合贝伐珠单抗对比TACE治疗中期HCC的Ⅲb期、随机、多中心、开放标签试验
英文标题:IKF-035/ABC-HCC: A phase Ⅲb, randomized, multicenter, open-label trial of atezolizumab plus bevacizumab versus transarterial chemoembolization (TACE) in intermediate-stage hepatocellular carcinoma
摘要号:478
研究背景
HCC是全球范围内最常见且致死率最高的恶性肿瘤之一。TACE作为局部治疗手段,是目前中晚期(BCLC B期)HCC的标准治疗方案。IMbrave150 Ⅲ期研究表明,对于TACE治疗失败或不适合TACE的晚期和中晚期HCC患者,抗PD-L1抗体阿替利珠单抗联合抗VEGF抗体贝伐珠单抗的一线治疗方案较索拉非尼可延长生存期,并因此被批准用于该适应症。然而,对于原本应按标准方案接受TACE治疗的中期HCC患者,阿替利珠单抗联合贝伐珠单抗是否优于TACE尚不明确。尽管已有若干试验正在评估TACE联合系统治疗对比单纯TACE的获益差异,但ABC-HCC试验直接比较了阿替利珠单抗联合贝伐珠单抗及系统治疗对比TACE的疗效和安全性。本研究采用分组序贯设计,计划在信息成熟度达到33%和66%时进行两次中期分析,以评估疗效/无效性。
研究方法
ABC-HCC是一项国际、多中心、随机、开放标签、由研究者发起的Ⅲb期临床试验,旨在直接比较阿替利珠单抗联合贝伐珠单抗对比TACE在中期HCC或经主治医师判断具有TACE适应证的HCC患者中的疗效。研究计划纳入320例确诊HCC患者,入选标准包括:不适合根治性手术/消融或肝移植,但适合TACE治疗;无肝外转移;无大血管侵犯(Vp1/2型门静脉侵犯除外);ECOG评分≤1;Child-Pugh分级为A级或B7级。患者按1:1随机分配接受系统治疗(A组:阿替利珠单抗,1200 mg静脉注射;贝伐珠单抗,15 mg/kg静脉注射;每3周一次;最长治疗24个月)或TACE治疗(B组:按需进行,由研究者评估认为可继续接受TACE时再进行)。每8周进行一次影像学检查(CT/MRI),以评估主要终点“治疗策略失败时间”(TTFS:从随机分组到死亡或需要其他治疗方案的时间)。本研究报告了在33%信息成熟度时进行的首次疗效/无效性中期分析结果。
研究结果
截至数据分析时,已在奥地利、法国、德国、印度、意大利、日本和西班牙的54个研究中心入组206例患者。在数据截止日期,共有194例患者完成随机分组,其中168例患者随访时间≥3个月,被纳入本次中期分析(A组:87例;B组:81例)。在主要终点TTFS方面,共记录到100起事件(A组:44例;B组:56例)。系统治疗组的中位TTFS为14.6个月,TACE治疗组为9.5个月(HR=0.55;95%CI:0.36~0.83)。基于上述结果,本研究将继续进行。
研究结论
首次中期分析的结果为评估阿替利珠单抗联合贝伐珠单抗对比TACE在中期HCC患者中的疗效提供了重要依据,并提示在TTFS方面,系统治疗可能优于TACE。基于该发现,本研究将推进至66%信息成熟度(169例事件)时的第二次中期分析[1]。
研究者说
关于IKF-035/ABC-HCC研究,亚组设计在入组时已考虑肿瘤负荷、病灶数量和肝功能分层等因素,这些信息将通过次要终点或描述性分析收集。对比TACE,阿替利珠单抗联合贝伐珠单抗在中期HCC患者中的主要临床获益,目前首次中期分析结果尚不完全,我们预期将在包括OS在内的终点中观察到优效性。基于现有结果,该研究可能促使临床实践中更多BCLC B期患者接受联合治疗。
研究二
中文标题:纳武利尤单抗联合伊匹木单抗对比仑伐替尼或索拉非尼一线治疗不可切除HCC:CheckMate 9DW试验的4年随访结果
英文标题:Nivolumab plus ipilimumab vs lenvatinib or sorafenib as first-line treatment for unresectable hepatocellular carcinoma (HCC): 4-year follow-up of CheckMate 9DW
摘要号:LBA479
研究背景
在CheckMate 9DW研究(NCT04039607)预先设定的中期分析中,中位随访35.2个月的结果显示,在未经治疗的不可切除HCC患者中,纳武利尤单抗联合伊匹木单抗(NIVO +IPI)较仑伐替尼或索拉非尼(LEN/SOR)显著延长了总生存期(OS)(HR=0.79;95%CI:0.65~0.96;P=0.0180),客观缓解率(ORR)更高(36% vs. 13%,P<0.0001),且缓解持续时间更长,安全性良好[2]。基于这些结果,NIVO+IPI联合方案已获得美国FDA、欧盟委员会及其他国家批准,作为不可切除HCC的一线治疗方案。本文报告了中位随访4年的最新疗效和安全性结果。
研究方法
本研究纳入经组织学确诊、既往未接受过系统治疗的晚期HCC成年患者,这些患者不适合接受或经根治性手术/局部区域治疗后疾病进展,根据RECIST v1.1标准,未治疗病灶≤1个,Child-Pugh评分为5或6分,ECOG体能状态评分为0或1分。患者按1:1的比例随机分组,分别接受NIVO 1 mg/kg+IPI 3 mg/kg每3周一次(最多4个周期)治疗,随后接受NIVO 480 mg每4周一次治疗,或由研究者选择SOR 400 mg每日两次或LEN 8 mg或12 mg每日一次治疗,直至疾病进展或出现不可耐受的毒性反应。NIVO的给药时间最长为2年。主要终点为OS;次要终点包括由盲态独立中心评估(BICR)的ORR和缓解持续时间(DOR)。
研究结果
共有668例患者随机分配至NIVO+IPI组(n=335)或LEN/SOR组(n=333);在LEN/SOR组的325例患者中,275例(85%)接受了LEN治疗。经过52.5(44.0~66.1)个月的中位随访后,NIVO+IPI方案与LEN/SOR方案相比,持续显示出OS获益(HR=0.78;95%CI:0.65~0.93),且48个月OS率更高(31% vs. 18%)。NIVO+IPI方案的ORR高于LEN/SOR方案(36% vs. 13%),完全缓解率也更高(分别为8% vs. 2%),且DOR更长(中位DOR分别为34.3个月 vs. 12.9个月)(表1)。治疗相关不良事件(TRAE)的汇总见表1。
表1. 研究结果
研究结论
经过4年的随访,一线NIVO+IPI方案在不可切除的HCC治疗中持续表现出优于LEN/SOR方案的疗效获益,且安全性可控,未出现新的安全性问题。上述结果进一步支持NIVO+IPI方案作为此类患者的标准治疗方案[3]。
研究者说
开展CheckMate 9DW研究并设置4年随访期,主要是考虑到目前仍有相当一部分患者对Imbrave150或Himalaya方案无应答,存在未被满足的临床需求。在长期随访中,纳武利尤单抗联合伊匹木单抗的关键生存数据显示,4年总生存率达31%,相较于对照组的18%表现突出。在安全性方面,未观察到新的不良事件,免疫相关不良事件通常较早发生,长期管理未见新增风险。这些长期结果进一步确认了该联合方案在不可切除HCC一线治疗中的良好疗效和可靠安全性,为临床实践提供了重要依据。
参考文献:
[1] Peter Robert Galle, et al. 2026 ASCO GI. Abstract 478.
[2] Yau T, et al. Lancet. 2025 May 24;405(10492):1851-1864.
[3] Peter Robert Galle, et al. 2026 ASCO GI. Abstract LBA479.
Abstract 478摘要原文
IKF-035/ABC-HCC: A phase Ⅲb, randomized, multicenter, open-label trial of atezolizumab plus bevacizumab versus transarterial chemoembolization (TACE) in intermediate-stage hepatocellular carcinoma
BACKGROUND:
Hepatocellular carcinoma (HCC) is among the most common and deadliest cancers worldwide. Locoregional treatment (LRT) with transarterial chemoembolization (TACE) is standard of care (soc) for intermediate stage (BCLC B) HCC. The IMbrave150 phase 3 study demonstrated that combination of the anti-PD-L1 antibody atezolizumab and the anti-VEGF antibody bevacizumab (atezo/bev) extends survival compared to sorafenib in first-line treatment of advanced and intermediate stage HCC failing/unsuited for TACE which has led to its approval in this setting. However, it is unknown if atezo/bev is more efficacious than TACE in patients with intermediate stage HCC patients who would be treated with TACE per soc. While several trials assess the benefit of adding systemic therapy to TACE vs. TACE alone, the ABC-HCC trial directly compares the efficacy and safety of systemic treatment with atezo/bev vs. TACE. ABC-HCC is using a group sequential design with two planned interim analyses (IA) at 33% and 66% information time to assess efficacy/futility.
METHODS:
ABC-HCC is an international phase 3b, randomized, multicenter, open-label, investigator-initiated trial directly comparing atezo/bev vs. TACE in intermediate stage HCC or HCC with indication for TACE according to the treating physician. 320 patients with confirmed HCC (not amenable to curative surgery/ablation, liver transplantation, but amenable to TACE, no extrahepatic spread, no macrovascular invasion except for Vp1/2, ECOG ≤ 1, Child-Pugh A/B7) are randomized (1:1) to receive either systemic treatment (Arm A: atezo, 1,200 mg IV; bev, 15 mg/kg IV; Q3W; max. 24 months) or TACE (Arm B: on demand as long as TACEable as assessed by the investigator). Imaging (CT/MRI) is performed Q8W to determine the primary endpoint time to failure of treatment strategy (TTFS: Time from randomization until death or need for a further therapeutic option). Here, we report on the first efficacy/futility IA at 33% information time (85 events).
RESULTS:
To date, 206 pts have been enrolled at 54 centers in Austria, France, Germany, India, Italy, Japan and Spain. At data cut-off (06/13/2025), 194 pts were randomized, of whom 168 pts had a follow up duration of ≥ 3 months and were included in the IA (Arm A: 87; Arm B: 81). 100 events were observed for the primary endpoint TTFS (Arm A: 44; Arm B: 56). Median TTFS was 14.6 months in Arm A vs. 9.5 months in Arm B with a HR of 0.55 (95% CI [0.36, 0.83]). Based on these results, the trial was continued.
CONCLUSIONS:
The results of the first IA provide important insights into the efficacy of atezo/bev vs. TACE in intermediate stage HCC and suggest a superiority of systemic therapy compared to TACE in regard to TTFS. Based on these findings, the trial is progressing to the second IA at 66% information time (169 events).
Abstract LBA479摘要原文
BACKGROUND:
At a preplanned interim analysis of CheckMate 9DW (NCT04039607), with 35.2 months of median follow-up, nivolumab plus ipilimumab (NIVO + IPI) demonstrated significant overall survival (OS) benefit vs lenvatinib or sorafenib (LEN/SOR) (hazard ratio [HR] 0.79 [95% CI, 0.65-0.96]; P = 0.0180), higher objective response rate (ORR; 36% vs 13%, P < 0.0001) with durable responses, and manageable safety in patients (pts) with previously untreated unresectable HCC (Yau T et al. Lancet 2025;405:1851-64). Based on these results, NIVO + IPI combination was approved as a first-line (1L) treatment for unresectable HCC by the US FDA, European Commission, and in other countries. We report updated efficacy and safety results at a median follow-up of 4 years.
METHODS:
Adults with previously untreated histologically confirmed advanced HCC, either ineligible for or having progressed after curative surgical/locoregional therapies, ≤ 1 measurable untreated lesion per RECIST v1.1, Child-Pugh score 5 or 6, and ECOG performance status 0 or 1 were included. Pts were randomized 1:1 to receive NIVO 1 mg/kg + IPI 3 mg/kg Q3W (up to 4 cycles) followed by NIVO 480 mg Q4W or investigator's choice of SOR 400 mg BID or LEN 8 mg or 12 mg QD until disease progression or unacceptable toxicity. NIVO was given for a maximum of 2 years. The primary endpoint was OS; secondary endpoints included ORR and duration of response (DOR) per blinded independent central review (BICR).
RESULTS:
A total of 668 pts were randomized to NIVO + IPI (n = 335) or LEN/SOR (n = 333); among 325 pts treated in the LEN/SOR arm, 275 (85%) received LEN. After a median (range) follow-up of 52.5 (44.0-66.1) months, NIVO + IPI continued to show OS benefit vs LEN/SOR (HR, 0.78; 95% CI, 0.65-0.93), with higher 48-month OS rates (31% vs 18%; Table). ORR was higher with NIVO + IPI vs LEN/SOR (36% vs 13%), with higher complete response rates (8% vs 2%, respectively) and durable responses (median DOR, 34.3 vs 12.9 months, respectively; Table). A summary of treatment-related adverse events (TRAEs) is shown in the Table.
CONCLUSIONS:
After 4 years of follow-up, 1L NIVO + IPI continued to show sustained efficacy benefit vs LEN/SOR in unresectable HCC and manageable safety with no new concerns. These results continue to support NIVO + IPI as a standard-of-care treatment in these patients.
- 推荐文章
Nature Medicine丨27万人大数据,瑞典SCREESCO试验证实开展CRC筛查能有效提升早癌检出率
英国获批!Zanidatamab为HER2高表达胆道癌患者带来精准治疗新选择
JCO重磅发表CHANCE2005/CARES-005研究!TACE联合靶免为不可切除HCC治疗带来新希望
Ann Oncol丨CheckMate 649研究5年随访结果:纳武利尤单抗联合化疗一线治疗晚期胃癌患者生存获益持久,安全性可控
心灵驿站丨当医生直面自身健康危机:在恐惧与希望交织中的探寻与顿悟
“瘤瘤”新知丨TP53状态如何左右一碳代谢相关营养素与结直肠癌风险关联的“天平”?
长期使用质子泵抑制剂真的会增加胃腺癌风险吗?近20万人随访26年的大数据给出新答案!
这几类癌症幸存者需警惕!既往肿瘤史成为影响食管鳞癌患者生存的重要因素!
《肿瘤瞭望消化时讯》给大家拜年啦!
除夕献礼!2025消化时讯十大年度热文盘点:致敬过往,共启新章
国产双抗Anbenitamab为HER2阳性胃癌后线治疗带来新希望:Ⅲ期KC-WISE研究的预设中期分析结果
JCO丨可切除及临界可切除胰腺癌围术期VTE发生率达9%,死亡风险翻倍
心灵驿站丨生死无言:一位医生与四代女性的未竟之语
JCO:JCOG0603研究长期随访结果发布,辅助mFOLFOX6未改善结直肠癌肝转移患者OS
岂有此“例”|晚期HCC能否“绝处逢生”?——肝静脉瘤栓+双肺转移患者经治生存14年的启示
JCO重磅:超600万人队列研究提示,年轻人群重度饮酒显著增加早发性胰腺癌风险
年度盘点丨胃肠研途,智领前沿——沈琳教授团队2025学术攻坚实录
系统评价与荟萃分析揭示围手术期免疫联合化疗为可切除胃/胃食管结合部癌患者带来明确获益
心灵驿站丨当医生成为生命重负的承载者:在生死交织中的坚守与思索
秦叔逵教授:2025胰腺癌诊疗进展盘点|2025肝胆胰肿瘤年终盘点暨第2届临床热词发布会
“瘤瘤”新知丨何时“动”起来最有益?研究揭示不同治疗阶段结直肠癌患者进行体力活动的“生存密码”
食管胃结合部腺癌根治术的前瞻性评估:CLAEG研究带来的真实世界见解
1/3的癌症可以预防!这份科学防癌行动清单要收藏丨世界癌症日
STTT丨文天夫教授团队合作取得新进展:仑伐替尼+经肝动脉化疗栓塞+PD-1单抗三联转化治疗可显著提高不可切除HCC转化手术率
mFOLFOXIRI联合帕尼单抗一线治疗不可切除RAS/BRAF野生型转移性结直肠癌:Ⅲ期TRIPLETE研究的最终结果
喜报!爱思唯尔2025年度“中国高被引学者”榜单揭晓,肿瘤领域百余位专家入选
惕这6类“促癌食物”,你可能每天都在吃!
最新研究揭示晚期HCC患者系统治疗模式的演变与生存现状
心灵驿站丨当医生成为临终患者见证者:一场身份交织下的感悟与思索
JCO丨许剑民教授牵头NEOTERIC研究新突破:双免新辅助治疗LARC,pCR率达35.7%!
最新研究显示新辅助放化疗联合手术与术后辅助放化疗在局部晚期食管鳞癌患者中的长期生存结局相当,个体化精准决策是关键
岂有此“例”|警报未解除:一例EOCRC患者根治术后11年罕见复发带来的长期随访启示
早期单发HCC一线治疗再评估:TACE联合放疗的获益人群和最佳时机
国之脊梁,风范永存:沉痛送别中国肿瘤内科学奠基人孙燕院士
ASCO GI现场|HCC术后辅助治疗受挫:KEYNOTE-937研究RFS结果阴性
ASCO GI国际视角|肝癌治疗进展速递:两项研究同证免疫联合方案治疗获益
ASCO GI大咖点评|陈功教授解读BREAKWATER研究:Encorafenib+西妥昔单抗+FOLFIRI方案一线治疗BRAF V600E突变型mCRC结局更优
ASCO GI中国之声|林榕波教授团队:替雷利珠单抗联合多药化疗治疗晚期胃癌的前沿进展
ASCO GI现场直击|国际视角:真实世界研究数据证实肝移植在不可切除结直肠癌肝转移治疗中的潜力
APTNM新分期:肿瘤标志物联合TNM分期,实现肝癌手术预后精准分层
“瘤瘤”新知丨警惕!溃疡性结肠炎伴背景黏膜炎症竟是结直肠癌患者不良预后“警报器”
ASCO GI现场直击|国际视角:精准医疗时代下的MRD检测新进展
ASCO GI中国之声|王峰教授:呋喹替尼联合特瑞普利单抗及SOX一线治疗晚期胃癌的数据更新
ASCO GI中国之声丨崔玖洁医生解读ALTER-PA-001研究:靶免联合一线治疗mPC,ORR达40%!
ASCO GI热评|可切除胃癌全程新辅助治疗显现潜力,聂润聪副主任医师解读CRITICS-Ⅱ研究
首项头对头随机研究揭示ESD vs. TAMIS治疗早期直肠肿瘤,ESD更具综合优势
ASCO GI大咖点评|李恩孝教授解读:两项亚洲研究聚焦免疫联合化疗(GCD)方案,全方位优化晚期BTC治疗策略
ctDNA作为早期临床研究的生物标志物:现状、挑战与未来展望
ASCO GI中国之声|胰腺癌治疗新路径:天肿两项Ⅱ期研究公布CLDN18.2联合疗法新数据
ASCO GI热点追踪|Ⅲ期COMMIT研究证实靶免化三联方案一线治治疗dMMR/MSI-H型mCRC患者,PFS显著优于免疫单药
ASCO GI中国之声|聂润聪副主任医师解读CAPITAL研究:SOX辅助治疗对比S-1改善Ⅱ~Ⅲ期胃癌长期生存
ASCO GI|可切除胃癌新辅助治疗策略探索:化疗序贯放化疗方案综合获益更优
ASCO GI热点追踪丨新方案,新突破:免疫联合PARP抑制剂在DDR突变型转移性胰腺癌中初显潜力
岂有此“例”|新辅助免疫治疗实现pCR:dMMR/MSI-H转移性结直肠癌的突破性病例分享
ASCO GI现场直击|魏嘉教授解读TERRIFIC研究:免疫联合放化疗在局晚期胃癌中显示出疗效获益